Access to SRHR Information and services
COMPREHENSIVE SEXUALITY EDUCATION
Despite the contentious debates surrounding the provision of comprehensive sexuality education to adolescents and youth, it is a globally recognized need and right of young people. This right has been recognized by various international human rights agreements, including but not limited to the Convention on the Rights of the Child, the International Covenant on Economic, Social, and Cultural Rights, and the Convention on the Elimination of All Forms of Discrimination against Women. However, in Asia, this need is, for the large part, unmet.
Sex education is defined as basic education about reproductive process, puberty, and sexual behavious.31 Comprehensive Sexuality Education (CSE), on the other hand, may incorporate other components of sexual and reproductive health and rights, including attitudes toward sexuality, gender relations, and information about services pertaining to sexual and reproductive health, such as contraception or HIV testing services.32 The importance of a comprehensive sexuality education program lies in its ability to create a safe and open environment for youths to learn and discuss their SRHR. It provides a gateway for adolescents to receive beneficial and accurate information, so that they are empowered to make an informed decision when the time calls for it. CSE is also an opportunity to create awareness of the services that are provided for them in exercising their SRHR, such as contraception, STI treatment and postpartum care, and it is also a medium by which we can address gender issues, including the alleviation of gender-based violence among young people.
The reasons for the lack of implementation of CSE in the region are complicated by various political, religious and social factors. Religious conservatism have restricted or eliminated CSE programmes in many communities.35 In the Asian region, Afghanistan, Bangladesh, Indonesia, Nepal and Thailand have national strategies that make direct reference to reproductive health in education, however, most of these countries have yet to formally employ CSE in their primary or secondary education curricula, potentially due to cultural or religious conservatisms .15 The lack of political will to overcome the challenges posed by religious and cultural fundamentalisms is the main reason for the lack of implementation of CSE in the region.
YOUTH-FRIENDLY SRHR SERVICES
Creating a youth-friendly environment in health care is key in enabling young people's access to these services. Sexual and reproductive health services for young people should be legal, non-discriminatory, accessible without restrictions on age and/or parental consent, affordable, and of high quality, to ensure that the rights of these individuals are protected. Sadly, the provision of youth-friendly services has taken a step back on national agendas. In many countries in Asia, youth-friendly clinics are provided by non-governmental entities, but the reach of these programmes are usually limited. Youth friendly SRHR services includes, but is not limited to, access to a wide range of contraception methods, access to safe abortion services, HIV treatment and care, counselling services, and many more.
Adolescent pregnancy rates can be greatly reduced with the uptake of contraception in Asia. Young people have the right to choose the timing and spacing of children, if they choose to have children. However, the full and free access to contraception by young people is often complicated by societal taboos and widespread lack of knowledge. The sensitivity of this topic is also reflected in the lack of data available on current contraceptive prevalence rates among adolescents and youth. In countries where premarital sex is prohibited by law, data on contraceptive access and use among unwed adolescents is non-existent. Even in the MDGs, the contraceptive prevalence rate for youth is subsumed under the overall prevalence rate of women of reproductive age, and this data is typically collected among married women. Only in the recent country Demographic Health Surveys are there age-disaggregated data on contraceptive prevalence rates, but again, the sample in many countries consists of married women only.
In Asia, Indonesia and Bangladesh observes the highest prevalence rates of contraceptive use, approximately 60% of married youth between 20 and 24 years old and 45% of married youth between 15 and 19 years old reported current use of contraception.16 For other Asian countries with available data, the contraceptive prevalence rate among youths is among the lowest in the Global South region. In Cambodia, for example, the contraceptive prevalence rate of any method among younger youths is only 2% and it is 19% for older youths.16 Considering that these data came primarily from the pool of married youth, it is alarming to note that there is such a high degree of lack of use among presumably sexually active young women. It is important to reiterate that these data only captures the prevalence of contraception use among married youths; data on contraceptive use in unmarried youth and those under 15 years of age are scarce.
CONTRACEPTION PREVALENCE RATES AMONG ADOLESCENTS AND YOUNG WOMEN
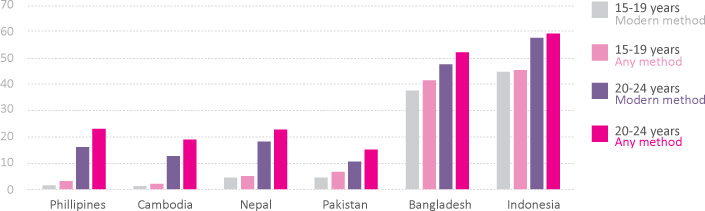
Figure 1: Contraceptive prevalence rates in countries where data was available16
The provision of safe abortion services for young people is also insufficient in this part of the world. In developing countries, adolescent girls account for over 2 million unsafe abortions yearly. However, unsafe abortion rates are predominantly estimates; there is no direct way to measure the extent of unsafe abortion among young women in a country, given the cloaked nature of these practices. In 2004, the WHO published estimates of unsafe abortion rates from 2000.17 According to this data, about 14% of unsafe abortions occur among women younger than 20. In Asia, these figures are over 30%. Evidence has shown that the risk of death due to abortion-related complications is highest for unmarried adolescents. 18In Asia, access to safe abortion services are hurdled by cultural stigmas and religious taboos, as well as legal barriers that stipulate age and term restrictions, as well as consent requirements.
These are just some of the barriers to SRHR services and information that young people face, leading them into the cycle, of early pregnancy and sexually transmitted infections, of discrimination and prejudice, and of gross violations of their sexual and reproductive health and rights. Changes in policy that fully protect these rights is a first, and important, step in reducing the burden of young Asians, and full implementation of these changes into effective programmes will change the course of these young lives.
BASED ON YOUNG PEOPLE'S EXPERIENCE IN ASIA, WE CALL ON GOVERNMENTS, NON-GOVERNMENTAL BODIES, YOUNG PEOPLE, AND OTHER STAKEHOLDERS TO:
1. Put youth at the center of all the processes, including in the planning, implementation, monitoring and evaluation stages, and at all levels, ranging from local, national, regional and global arenas.
2. Prioritize the adoption and successful implementation of evidence-based, universally accessible, quality, nonjudgmental comprehensive sexuality education in a safe and participatory environment that caters to formal, informal, and non-formal education systems.
3. Prioritize the implementation of youth-friendly services that is high quality, integrated, equitable, comprehensive, affordable, needs and rights based, accessible, acceptable, confidential, and free of stigma and discrimination for all young people, in alignment with international standards
4. Ensure that young people have comprehensive information about and access to a choice of the widest possible range of safe, effective, affordable and acceptable modern methods of contraception, including both long-term and short-term methods.
5. Provide access to safe abortion information and services and remove barriers such as gestational limits, parental/ spousal consent, mandatory waiting periods and counseling.
6. Enact and strictly enforce laws to ensure that marriage is entered into only with the free and full consent of the intending spouses. Laws concerning the minimum legal age of marriage should be raised, where necessary, to meet the requirements of previously ratified international agreements.
7. Tighten and fully implement laws that restrict traditional practices that are harmful to adolescents and young people, including the practice of FGM and honor killings.
8. Scale up efforts to meet the goal of ensuring universal access to HIV prevention, treatment, care and support, free of stigma and discrimination and with a gender perspective, and to provide comprehensive information, voluntary counseling and testing to adolescents and youths living with HIV.
9. Monitor the status of young people's SRHR in order to identify gaps and formulate effective intervention strategies. Data collected should be disaggregated and represent the diversity of young people, so that the specific needs of particular sub-groups can be addressed.